ORIGINAL RESEARCH ARTICLE
Relationship of tumor necrosis factor super family member 4 (TNFSF4) gene SNP rs505922 with atherosclerotic cerebral infarction in Tengzhou region
Song Zhengfeng
1,2, Deqin Geng
1*, Xu Yan
3, Qi Peng
2
1Graduate School of Xuzhou Medical College, Jiangsu, People’s Republic of China
2Department of Pediatrics, Tengzhou Central People’s Hospital, Tengzhou, People’s Republic of China
3Department of Neurology, Xuzhou Medical College Affiliated Hospital, Jiangsu, People’s Republic of China
Abstract: The aim of the study is to investigate the relationship between the incidence of atherosclerotic cerebral infarction and tumor necrosis factor super family member 4 (TNFSF4) on the upper point of the gene and the gene frequency SNP rs505922 polymorphism. 185 patients with atherosclerotic cerebral infarction in a local household registration hospital were selected from January 2012 to January 2013. 180 cases for routine checks in our hospital were selected as the control group. The polymorphism and gene frequencies of SNP rs505922 on TNFSF4 were detected by polymerase chain reaction assay. The rs505922 genotype and allele frequency analysis revealed that C allele frequency in the atherosclerotic cerebral infarction group was higher than that in the control group; the difference was statistically significant (
P < 0.05). CC genotype is an independent risk of atherosclerotic cerebral infarction risk factors. In conclusion, the upper point TNFSF4 gene SNP rs505922 CC genotype was closely related with local atherosclerotic cerebral infarction.
Keywords: atherosclerotic cerebral infarction; tumor necrosis factor superfamily member 4; SNP rs505922 gene
Citation: Zhengfeng S et al, Relationship of tumor necrosis factor super family member 4 (TNFSF4) gene SNP rs505922 with atherosclerotic cerebral infarction in Tengzhou region. J Gen Neuro 2016; 1(1):
*Corresponding author: De-qin Geng, Graduate School of Xuzhou Medical College, Jiangsu, 221004, People’s Republic of China, gengdeqin@126.com.
Introduction
At present, many researchers agreed that genetic and environmental factors play an important role in the development process in cerebral infarction, but its pathogenesis still remains unclear
[1]. Cerebral infarction can be divided into atherosclerotic cerebral infarction and lacunar cerebral infarction on the basis of different causes
[2]. Atherosclerosis cerebral infarction refers to cerebral infarctions that appear on the basis of cerebral atherosclerosis vascular lesions such as vascular stenosis, occlusion and thrombosis that are caused by cerebral infarction in corresponding blood vessels. Lacunar cerebral infarction refers to the cerebral hemisphere or deep perforating arteries of the brain stem (100–200 µm in diameter), on the basis of long-term high blood pressure, blood vessel walls lesions would occur, causing luminal occlusions and small brain infarctions. According to Gu et al., atherosclerosis is the most common cause of cerebral infarction; tumor necrosis factor super family member of 4 (TNFSF4) gene’s polymorphism and the development of atherosclerosis are closely related; rs505922 is the important regulating site on TNFSF4; the relationship between rs505922 gene’s polymorphism and frequency and the atherosclerotic cerebral infarction incidence is unknown
[3]. For these reasons, this article aimed to detect the rs505922 gene among regional atherosclerosis cerebral infarction, and compare it with healthy individuals in order to provide a new research idea for screening high-risk patients with cerebral infarctions.
Materials and methods
Equipment and materials: PCR Automatic Amplifier (GeneAmp PCR System 3700, PerkinElmer
®, USA), DNA Sequencing machine (ABI PRISM® 3700 DNA Analyzer 377, Applied Biosystems
™, USA).
Research subjects and grouping: 185 cases of local household registration of ischemic cerebral apoplexy patients treated at the Central People’s Hospital Neurology Department in Tengzhou, Shangdong province between January 2012 and December 2012. 98 male, 87 female aged from 38 to 75 years old with an average age of 63.52 ± 4.36. 88 cases were of atherosclerosis cerebral infarction, and 97 cases were of lacunar cerebral infarction. 180 cases grouped as control were of Tengzhou, Shandong province’s household health checks; 92 male and 88 female cases aged 22 to 76 years old with an average age of 61.22 ± 9.41.
The standard set for grouping: Inclusion criteria: (1) All cases were with typical clinical manifestations screened by craniocerebral CT and/or MRI diagnosis, in line with the 2010 session of the national ninth cerebrovascular revision of the diagnostic criteria
[4]; (2) Patients with heart, head and blood-vessel related diseases, as well as relating to liver and renal function were ruled out in the control group which consisted of normal, healthy patients going for their check-up.
Exclusion criteria: Patients with incomplete liver and kidney functions, severe heart failure, increased intracranial pressure, pneumothorax, shock, thoracic trauma, cardiac, arteritis, drugs, tumor, brain aneurysms, vascular malformations caused by cerebral infarction.
Data collection: To collect two groups of subjects’ gender, age, BMI, history of coronary heart disease history, history of hypertension, diabetes mellitus, history of tobacco use, alcohol consumption, FPG, TC, LCL - C, TG, HCL-C and other indicators.
There were no significant differences on the average age and gender compositions between the ischemic stroke group and the control group. However, the ischemic stroke group had more proportion of patients with high blood pressure, diabetes, coronary heart disease, triglycerides, total cholesterol and other risk factors than the control group (
P < 0.05) (
Table 1).
TNFSF4 Genetic type detection[5]
After morning fast, 2 mL venous blood were taken from patients, put into EDTA anticoagulant tubes and stored at -20°C for later use. Blood genomic DNA extraction kits were used to extract the DNA for DNA Polymerase Chain Reaction (PCR) primer application. Oligo and Premier software
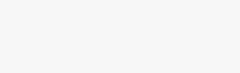
[12]were used to design the primers used (Sangon Biological Engineering, Shanghai): Upstream: 5’- GAGCCAAGACTTGTCCCCGG - 3’, Downstream: 5’- GAGCCAAGACTTGTCCCCGA - 3’. Amplification reaction system (25 µL): 2× Taq Master Mix 12.5 µL, 1 µL primers for upstream and downstream respectively, 3 µL DNA, deionized water 7.5 µL. Reaction conditions: 94°C denaturation for 3 min, 30 cycles of 94°C denaturation for 30 s, 30 s at 60°C for annealing, 72°C extension for 1 min; and finally 72°C for 10 min. The PCR product was detected using 2% agarose gel electrophoresis at 120V for 30–40 min. Amplification product size of 245 bp was observed from the gel electrophoresis image (
Figure 1).
PCR products enzyme reaction system (20 µL): 8 µL PCR products, 2 µL NIa Ⅲ,
BtsI µL [AR1] and 9.5 µL deionized water. The reaction was run in a 55°C water bath for 1 hour and the products were visualized using polyacrylamide gel electrophoresis at 220V (220–220 min, fixed, dyeing, color, gel image analysis) (
Figure 1).
Statistical analysis
The results of the experiment were analyzed using SPSS19.0 software analysis, measurement data using mean standard deviation (+ / - s), comparison between measured data sets using
t-test, χ
2 test between count data sets, Pearson single factor analysis, multiple factors Logistic analysis, with
P < 0.05 as statistically significant.
Results
1. Ischemic stroke subtype group compared with control group genotypes and alleles
In 185 cases of acute cerebral infarction group, there were 88 cases of atherosclerosis cerebral type (CT) infarction subtypes and 97 cases of lacunar cerebral infarction (LI) subtypes. Atherosclerosis in patients with cerebral infarction group CC, CT proportion and, C allele frequency was higher than the control group, and the difference was statistically significant (
P < 0.05). The lacunar cerebral infarction group however, when compared with the control group, CC, CT proportion and C allele frequency was not statistically significant (
P > 0.05) (
Figure 3).
2. Gene TNFSF4 rs505922 genotypes and correlation with atherosclerosis cerebral infarction
Taking atherosclerotic cerebral infarction as dependent variables; genotypes (CC, CT, TT), BMI, history of coronary heart disease, hypertension, diabetes mellitus, tobacco use, alcohol consumption, FPG, TC, LCL-C, TG, HCL-C as independent variables, the Logistic multivariate analysis showed that the CC genotype, history of hypertension, coronary heart disease history, diabetes history were independent risk of atherosclerosis, among which the highest risk being the CC genotype (OR:4.986, 95% CI: 1.232–7.025) (
Table 3)
[AR2] .
Discussion
Cerebral infarction is a disease mainly affecting the elderly and is caused by many factors like genetics and the environment with high mortality and morbidity
[6].
A large number of epidemiological and etiological research suggested that genetics played a vital role in the occurrence of cerebral infarctions. It was recently suggested that the human TNFSF4 gene mutation is inextricably linked with the occurrence and development of atherosclerosis
[5,7,8]. Gene TNFSF4 is also called the tumor necrosis factor ligand superfamily member 4 of about 23.60 kb located in lq25; has 3 exons; codes for the OX40L protein (also called OX40 Ligand, CDl34L, GP34, TXGPI). OX40L proteins are mainly expressed in dendritic cells, B lymphocyte and vascular endothelial cells, and CD40 signals can promote its expression
[9]. OX40L can bind with OX40 receptors of T lymphocytes, stimulating signals, eventually leading to the proliferation and differentiation of T lymphocytes; participating in memory CD4+ T cell’s differentiation and maturation; mediating T cell to inflammatory infiltrates
[10,11].
OX40L is TNFSF4 gene’s encoding protein; OX40L can encode B lymphocytes, dendritic cells, endothelial cells, macrophages, and some tissue cells. Sun et al. indicated that OX40L can participate in atherosclerosis by promoting T lymphocyte functions
[12]. An
in vitro experiment on mice on a high-fat diet showed that TNFSF4 genotype mice were more likely to develop atherosclerosis as compared to non-TNFSF4 genotype mice, thus inferring that TNFSF4 potentially existed in the control area and a single nucleotide polymorphism could affect its potential gene expression, affecting atherosclerosis
[13]. At present, a lot of
in vitro animal experiments have confirmed that TNFSF4 currently affects the susceptibility of atherosclerosis genes. Su et al. studied the connection of myocardial infarction and normal people, the result showed that TNFSF4 SNP rs505922 patients were more likely to exhibit myocardial infarctions
[14]. Wang et al. discovered that patients carrying the TNFSF4 SNP rs505922 genes with type 2 diabetes, were significantly more prone to atherosclerosis and plaque formation than SNP rs505922 carriers
[15].
Rs505922 is located in the third intron of TNFSF4. This study discovered that TNFSF4 SNP rs505922 polymorphism may participate and play a vital role in the onset of cerebral infarction in patients of Tengzhou, Shandong province. In this research, both the control group patients and atherosclerotic cerebral infarction group had three genotypes of CC, CT and TT, two groups of rs505922 gene polymorphism were in Hardy-Weinberg equilibrium prompting that the samples were from the same population. Gene frequencies representing the atherosclerotic cerebral infarction group’s distribution of the C allele frequency was higher than the control group, and the difference was statistically significant (
P < 0.05), suggesting that rs505922 may be closely related to the regional atherosclerosis cerebral infarction incidence. Thus it can be can deduced that base substitution can affect TNFSF4's gene promoter and mRNA expression, enhancing the expression levels of OX40L in some way thereby activating OX40L signal pathways. The enhanced expression level of T cells in the body stimulated the body to release a variety of cytokines, mediating the body’s various inflammatory responses and promoting the formation of atherosclerosis.
By analysing Logistic multifactors, the CC genotype is an independent risk factor for atherosclerotic cerebral infarction. Recent studies have pointed out that coronary heart disease (CHD) soluble OX40L were significantly higher than that of healthy people thus inferring that rs505922 can affect the plasma level of soluble OX40L, promoting atherosclerosis and increasing the risk of cerebral infarction by regulating gene function. This study found that, patients with the CC genotype were more prone to have atherosclerosis cerebral infarction. We should encourage clinical prevention and treatment of cerebral infarction to reduce the incidence and morbidity relating to atherosclerosis cerebral infarction. From what has been discussed, SNPS rs505922 CC genotype located on TNFSF4 is closely related to atherosclerosis cerebral infarction incidence in Tengzhou, Shandong province; SNP rs505922 C allele can be used as an independent risk factor of atherosclerosis cerebral infarction. Considering the limited sample size of this study and the ethnic and regional differences in the correlation of genes and diseases, further studies with a sample size encompassing different regional populations would be needed to identify the pathogenesis of ischemic cerebral apoplexy in relation to TNFSF4.
References
-
Yang LB, Li SL, Tan Y, Xu SF, Duan XM, et al. Relationship between high-expressed TL1A and level of IFN-γ secreted by T cells in acute stage of Guillain-Barr(e) syndrome.Chinese Journal of Neurology 2009; 42(10): 689–693.
-
Wang WZ. Neurology. 5th ed. Beijing: People’s Medical Publishing House; 2004.
-
Gu SM, Wei M, Zhang YY, Shao J, Li Q, et al. Gene expression of tumor necrosis factor superfamily in peripheral blood mononuclear cells during chronic heart failure. Chinese Heart Journal 2005; 17(5): 453–457.
-
Guidelines writing group for Neurology branch of Chinese medical association of cardiovascular epidemiology group of acute ischemic stroke. Guidelines for Acute Ischemic Stroke in China 2010.Chinese Journal of Neurology 2010, 43(2): 146–153.
-
Miura S, Ohtani K, Numata N, Niki M, Ohbo K, et al. Molecular cloning and characterization of a novel glycoprotein, gp34, that is specifically induced by the human T-cell leukemia virus type I transactivator p40tax. Mol Cell Bio 1991; 11(3): 1313–1325. doi: 10.1128/MCB.11.3.1313.
-
Li H, Luo YK, Ye QF, Ming YZ. Role played by TRAIL and its receptor DR4/DR5 in acute kidney transplantation rejection. China Medical Engineering 2005; 13(1): 1–3.
-
Soroosh P, Ine S, Sugamura K, Ishii N. OX40-OX40 ligand interaction through T cell-T cell contact contributes to CD4 T cell longevity. J lmmunol 2006; 176(10): 5975–5987. doi: 10.4049/jimmunol.176.10.5975.
-
Lane P. Role of OX40 signals in coordinating CD4 T cell selection, migration, and cytokine differentiation in T helper (Th)l and Th2 cells.J Exp Med 2000; 191(2): 201–206.
-
Wang GM, Yang Y, Jin YZ, Li AL, Hao J, et al. Blockade of both CD28/B7 and OX40/OX40L co-stimulatory signal pathways prolongs the survival of islet xenografts. Transpl P 2005; 37(10): 4449–4451. doi: 10.1016/j.transproceed.2005.10.117.
-
Fujita T, Kambe N, Uchiyama T, Hori T. Type I interferons attenuate T cell activating functions of human mast cells by decreasing TNF-α production and OX40 ligand expression while increasing IL-10 production. J Clin Immunol 2006; 26(6): 512–518. doi: 10.1007/s10875-006-9043-1.
-
Chen AI, McAdam AJ, Buhlmann JE, Scott S, Lupher ML Jr, et a1. OX40-ligand has a critical costimulatory role in dendritic cell: T cell interactions. Immunity 1999; 11(6): 689–698. doi: 10.1016/S1074-7613(00)80143-0.
-
Sun ST, Yang HY, Lou J, Chu M, Zhang JR, et al. Construction of expression vector with human costimulatory molecules 4-1BBL and its stable expression in Tca8113 cells.China Journal of Oral and Maxillofacial Surgery 2008; 6(3): 188–193.
-
Li J, Chen J, Song W, Bian Y, Yu H, et al. The case-control study between TNFSF4 polymorphism and coronary heart disease (CHD). Molecular Cardiology of China 2008; 8(1): 48–51.
-
Su R, Li J, Bian Y, Li M, Chen J, et al. The correlation of OX40 ligand protein gene polymorphisms and hypertension research. Chinese Journal of Integrative Medicine on Cardio/Cerebrovascular Disease 2010; 8(3): 274–276.
-
Wang K, Wang X, Wang Y, Zhang D, Zuo S, et al. Research on patients with coronary heart disease (CHD) OX40 ligand protein gene polymorphisms. Chinese Journal of Clinical Cardiology 2010; 26(12): 955–957.
TABLES
Table 1 Clinical data of the ischemic stroke and control groups
|
General Situation |
Ischemic stroke group (n=185) |
Control group
(n=180) |
χ2/t |
P value |
|
Gender (Male/Female) |
98/87 |
98/82 |
0.712 |
0.396 |
|
Average age |
63.52 ± 4.36 |
62.89 ± 3.45 |
0.326 |
0.712 |
|
Coronary heart disease |
22 (11.89%) |
2 (1.08%) |
8.263 |
0.000 |
|
Diabetes |
26 (14.05%) |
2 (1.08%) |
7.962 |
0.000 |
|
Tobacco use history |
98 (52.97%) |
32 (17.30%) |
9.123 |
0.000 |
|
Alcohol use history |
102 (55.14%) |
27 (14.59%) |
10.145 |
0.000 |
|
BMI (kg/m2) |
27.26 ± 2.18 |
24.98 ± 2.36 |
4.265 |
0.007 |
|
FPG (mmol/L) |
6.32 ± 1.85 |
5.23 ± 0.98 |
4.985 |
0.006 |
|
TC (mmol/L) |
4.98 ± 0.87 |
4.21 ± 0.96 |
5.262 |
0.003 |
|
TG (mmol/L) |
2.65 ± 0.45 |
1.02 ± 0.37 |
5.142 |
0.004 |
|
LCL-C (mmol/L) |
2.98 ± 0.58 |
2.02 ± 0.32 |
5.986 |
0.000 |
|
HCL-C (mmol/L) |
1.07 ± 0.75 |
1.39 ± 0.41 |
5.023 |
0.008 |
Table 2 Ischemic stroke subtype group rs505922 genotype and gene frequency analysis
|
Category |
Genotype [case (%)] |
Allele frequency |
Genotype |
Allele frequency comparison |
|
Group |
(n) |
CC |
CT |
TT |
C |
T |
χ2 |
P |
χ2 |
P |
OR |
(%) |
CI |
|
(CT) |
88 |
33 (37.50) |
46 (52.27) |
9 (10.23) |
|
0.892 |
9.123 |
0.000 |
5.693 |
0.013 |
1.185 |
95% |
0.936–3.245 |
|
(LI) |
97 |
5 (5.15) |
12 (12.37) |
80 (82.47) |
0.182 |
0.824 |
1.695 |
0.102 |
1.245 |
0.321 |
1.245 |
95% |
1.145–3.696 |
|
Control |
180 |
12 (6.67) |
20 (11.11) |
148 (82.22) |
0.185 |
0.815 |
|
|
|
|
|
|
|
Table 3 Logistic analysis of atherosclerotic cerebral infarction risk factors
|
Risk factors |
Regression
coefficient |
OR (95% CI) |
P value |
|
CC |
1.325 |
4.986 (1.232–7.025) |
0 |
|
CT |
1.428 |
3.425 (1.563–4.252) |
0.058 |
|
TT |
1.396 |
1.258 (0.963–4.158) |
0.063 |
|
High blood pressure |
1.262 |
4.125 (1.136-5.912) |
0.012 |
|
Coronary heart disease |
1.189 |
3.785 (1.063–5.126) |
0.015 |
|
Diabetes |
1.525 |
3.458 (1.063–5.023) |
0.019 |
|
Tobacco use history |
1.325 |
1.345 (1.152–6.023) |
0.068 |
|
Alcohol consumption history |
1.316 |
1.258 (0.856–5.102) |
0.071 |
|
FPG |
1.242 |
1.312 (1.023–5.639) |
0.075 |
|
TC |
1.278 |
1.212 (1.102–5.412) |
0.079 |
|
TG |
1.112 |
1.362 (1.245–6.325) |
0.085 |
|
LCL-C |
1.028 |
1.247 (1.045–6.102) |
0.091 |
|
HCL-C |
1.013 |
1.158 (0.912–6.352) |
0.093 |

FIGURE
Figure 1 Polyacrylamide gel electrophoresis visualization of TNFSF4 gene extron Rs505922 digested by NIa III. Marker: 50–450 bp DNA ladder; lanes 1–6: experimental group; lanes 7–12: control group